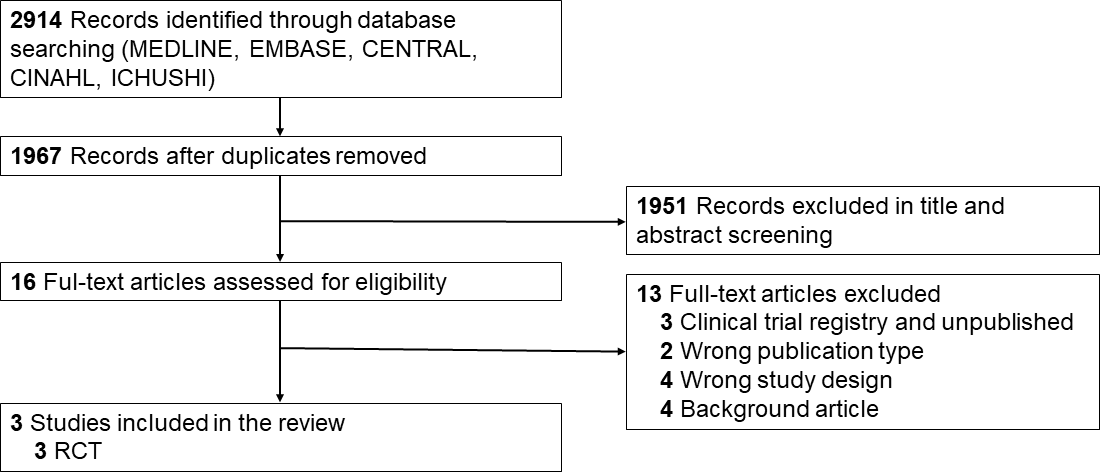
Objective: This study aimed to investigate the efficacy and safety of prophylactically administered sildenafil during the early life stages of preterm infants to prevent mortality and bronchopulmonary dysplasia (BPD). Data Sources: MEDLINE, Embase, Cochrane Central Register of Controlled Trials, Cumulative Index to Nursing and Allied Health Literature, and Ichushi. Study Selection: Published randomized controlled trials (RCTs), non‐RCTs, interrupted time series, cohort studies, case–control studies, and controlled before‐and-after studies were included. Data Extraction: Two reviewers independently screened the title, abstract, and full text, extracted data, assessed the risk of bias, and evaluated the certainty of evidence (CoE) following the Grading of Recommendations Assessment and Development and Evaluation approach. The random‐effects model was used for a meta‐analysis of RCTs. Results: This review included three RCTs (162 infants). The prophylactic sildenafil and placebo groups demonstrated no significant differences in mortality (risk ratio [RR]: 1.32; 95% confidence interval [CI]: 0.16–10.76; very low CoE) and BPD (RR: 1.20; 95% CI: 0.79–1.83; very low CoE), as well as in any other outcome assessed (very low CoE). Limitations: The sample sizes were less than the optimal sizes for all outcomes assessed, indicating the need for further trials. Conclusions: The prophylactic use of sildenafil in individuals at risk of BPD did not indicate any advantageous effects in terms of mortality, BPD, and other outcomes, or increased side effects.