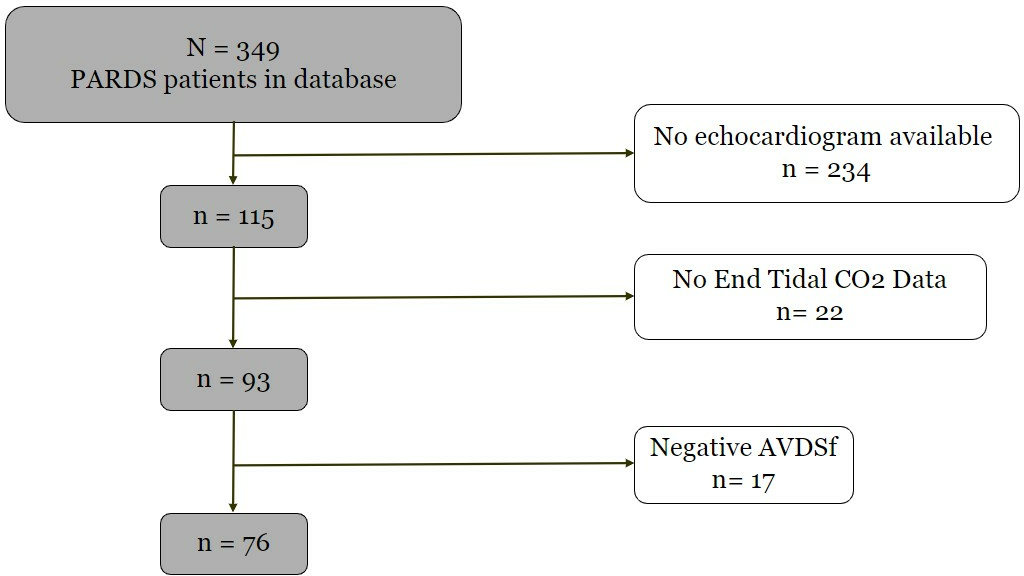
Primary Hypothesis: We hypothesized that higher alveolar dead space fraction (AVDSf) at PARDS onset would be associated with right ventricular (RV) systolic dysfunction within the first 24 hours of PARDS. Study Design and Methods: We performed a retrospective single-center cohort study of PARDS patients with clinically obtained echocardiograms within 24 hours. Primary exposure was AVDSf at PARDS onset. Primary outcome was RV systolic dysfunction as defined by RV global longitudinal strain (GLS) (> - 18%). Secondary outcomes included pulmonary hypertension (PH) and RV systolic dysfunction as defined by other echocardiogram parameters, and measures of oxygenation. Unadjusted and adjusted logistic and linear regression were used to investigate AVDSf associations with outcomes. Results: Seventy-six patients were included: median age 6.2 years, 50% female, and 66% with moderate or severe PARDS. Median AVDSf was 0.2 (IQR 0.1-0.3), 32% had RV dysfunction, and 24% had PH. Unadjusted and adjusted logistic regression showed no association between AVDSf and RV systolic dysfunction or PH by any echocardiographic measure. Unadjusted and adjusted linear regression demonstrated the association of AVDSf with both oxygenation index and PaO 2/FiO 2. AVDSf did not discriminate RV dysfunction (AUROC for RV GLS was 0.51, 95% CI 0.36-0.66). Conclusion: AVDSf at PARDS onset was not associated with RV systolic dysfunction or PH within 24 hours but was associated with metrics of hypoxemia and may be more reflective of pulmonary causes of ventilation-perfusion mismatch. Future investigations should focus on clarifying the clinical utility of AVDSf in relation to existing metrics throughout the course of PARDS.