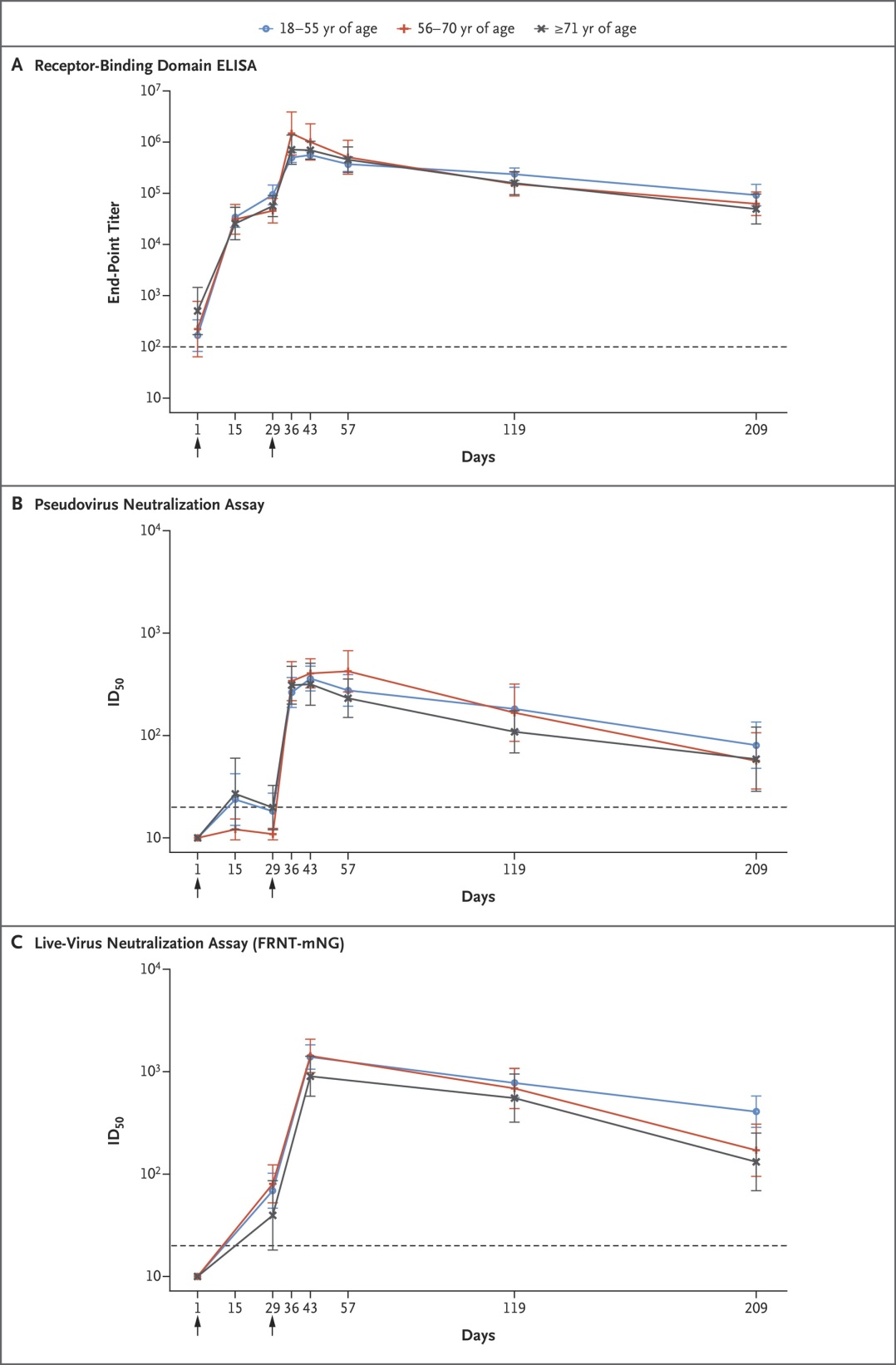
IntroductionWhether one has been infected with SARS-CoV-2 or had the Covid-19 vaccine, a robust innate and adaptive immune response is elicited. Recent studies provide evidence that the adaptive immune response can persist at high levels for over 6 months after vaccination as measured by sera antibody titers (Doria-Rose et al, 2021). Sera antibody titers against the SARS-CoV-2 virus are significantly higher in the vaccinated compared to those who are infected (Assis et al, 2021; Bartsch et al, 2021). For an unknown number of people, either of these events may lead to autoimmune disease (Guimarães et al, 2015); here called SARS-CoV-2 induced autoimmune disease (Ehrenfeld et al, 2020), and Covid-19 vaccine induced autoimmune disease (Toussirot and Bereau, 2015; Segal and Shoenfeld, 2018). While the two conditions may share similar mechanisms of an impaired, hyper immune response, long Covid may have additional mechanisms such as viral persistence (Wang et al 2020; Neurath et al, 2021). Viral persistence, even at low levels, can lead to a number of consequences, including the release of miRNA packaged into exosomes that induces a pro-inflammatory, Warburg-like effect in surrounding cells (Yoshikawa et al, 2019; Proal and VanElzakker, 2021). Common to both conditions, i.e vaccine induced and Covid-19 induced autoimmunity, susceptibility to infection or severe outcomes may include the effects of previous infections or vaccinations. For example, superantigen-mediated T cell activation can trigger broad B cell activation, and production of autoantibodies against a range of tissues has been shown in multi-inflammatory syndrome (Consiglio et al, 2020), and in patients with acute COVID-19. The spike protein, whether a part of the virion or of the Covid-19 vaccine, contains a superantigenic motif known to elicit a hyperinflammatory adaptive immune response (Cheng et al, 2020). Evidence also finds that the spike protein drives NLRP3 inflammasome activation in human microglia (Albornoz et al, 2022), a possible mechanism in developing neurological symptoms following Covid-19 infection or vaccination. One explanation for this happening is that the virus, or vaccine related proteins, can now target vascular endothelial cells and disseminate to the CNS through a hematogenous mechanism. Once at the blood-brain-barrier (BBB), SARS-CoV-2 or vaccine related protein, binds the zonulin receptor and promotes zonulin release. Then zonulin, via PAR2, induces blood-brain-barrier (BBB) disruption allowing the virus or protein to enter. Disruption of barrier function in epithelial and endothelial cells has been found by UC Berkeley scientists to be mediated by the spike protein alone (Biering et al, 2022), meaning that the spike protein made by mRNA vaccines can mediate this disruption of barrier function. Further, PEG has never been used in an approved vaccine until the mRNA vaccines, and its presence in Pfizer-BioNTech and Moderna-1273 vaccines has raised concerns about possible anaphylactic and fusogenic adverse effects (Sfera et al, 2022). Another concern is that PEG promotes temporary permeabilization of the BBB, a property used by the pharmaceutical industry for drug delivery to the CNS (Rabenel et al, 2020). This may account, in part, for the VAERS-reported neuropsychiatric symptoms, including neurodegenerative disorders (Frontera et al, 2022). Many excipients other than PEG are also used in the mRNA vaccines, and they too may be causative for adverse events (Borgsteede et al, 2021).Also, chronic activation of the immune system by viral persistence (or vaccine persistence, depending on how long the spike protein is made) can induce autoimmune responses, and molecular mimicry between components of a pathogen and host tissue can lead to specific post-infectious autoimmunity. Structural similarity between human neuronal antigens and SARS-CoV-2 proteins exists. A particular form of autoimmunity described in long COVID is postural orthostatic tachycardia syndrome, a form of autonomic dysregulation that is possibly induced by functional autoantibodies that target G protein–coupled receptors on neurons (Brodin et al, 2022). Another type of autoimmunity relevant to SARS-CoV-2 infection is the production of neutralizing autoantibodies to type I interferons, explaining a sizeable fraction of cases of hypoxemic COVID-19 pneumonia (Bastard et al, 2021). If such neutralizing autoantibodies are present before SARS-CoV-2 infection, due to prior infections or vaccinations, then a patient is clearly at risk of developing severe acute COVID-19 or vaccine induced autoimmune disease. Neutralizing autoantibodies may also appear after SARS-CoV-2 infection, in which case they might instead enable viral persistence, the formation of a viral reservoir and long COVID.Maguire (2022) has suggested a means to develop vaccines that better prevents the spread of virions and also reduce the probability of vaccine injury. However, current Covid-19 vaccine induced autoimmune disease can be severe in adults (de Brujin et al, 2021; Kaulen et al, 2022) and children (Buckhorn et al, 2021), leading to hospitalization. Life threatening autoimmune disease from Covid-19 vaccination has been successfully treated with a combination of 1. plasma exchange to clear autoantibodies from the blood, 2. Corticosteroids to reduce inflammation, 3. Rituximab to deplete beta cells, and 4. Caplacizumab an anti-von Willebrand factor to clear blood clots (de Bruijn et al, 2021).Autoimmune encephalitidies ((Zlotnik et al, 2021), venous sinus thrombosis (Finisterer and Nics, 2021; Sharifian-Dorche et al, 2021), intracranial hemorrhage with venous sinus thrombosis occurring in the same patient (Purkayastha et al, 2021), and glial fibrillary acidic protein astrocytopathy (GFAP-A) can result following the second dose of an mRNA vaccine (Koh et al, 2022). Autoimmune encephalitis is difficult to diagnose with current clinical diagnostics and therefore often goes untreated (Graus et al, 2016). Autoantibodies can persist for at least 6 months following even mild Covid-19 disease (Liu et al, 2021; Su et al, 2022). Neurological symptoms will result (Patone et al, 2021; Finisterer, 2022), including memory and attention deficits for up to 9 months (Zhao et al, 2022), and brain autoimmunity with attack of myelin in neurons may result (Gupta and Weaver, 2021; Shabani, 2021). Autoantibodies acting on vascular endothelial cells (Bouillet et al, 2013) in the part of the blood supply that feeds the brain, can cause thrombotic thrombocytopenia (Zuo et al, 2020; Gunther et al, 2021), and cerebral venous sinus thrombosis (Finsterer, 2021), and may also underlie the generalized report of “brain fog” in such patients and other forms of encephalopathy (Huang and Huang, 2022). Recent studies have found that spike proteins in SARS-CoV-2 attach to vimentin (Amraei et al, 2022), which is present at the extracellular surface of endothelial cells. This is a possible mechanism underlying the vaccine induced vascular abnormalities. Autoantibodies are also known to attack neutrophils, a key component of the innate immune response, and therefore could be an important reason for severe Covid-19 in those with autoimmune disease, potentially even that induced from vaccination (Weiner and Segelmark, 2016). Douaud et al (2022) found that Covid-19 whether severe or non-severe (not hospitalized), have significant brain damage. Whether this brain damage is the result of a hyperimmune response is not known, and therefore whether a hyperimmune response to vaccination could be resulting in the same brain damage is not known. However, because many of those autopsied after Covid-19 with CNS symptoms have not been found to have virions in their brain tissue, but do have immune cells present, a hyperimmune response is likely causative (Matschke et al, 2020). Concerning too is that mRNA vaccines may introduce DNA into the host genome, thus potentially introducing viral proteins to the host immune system for extended periods. Unlike what physicians in the media have said (Offit, 2021), humans possess robust reverse transcriptase enzymes that can write RNA sequences into DNA (Chandramouly et al, 2021), and the possibility exists that mRNA vaccines may introduce a DNA message into human genomes (Zhang et al, 2021; Alden et al, 2022). More work is required to provide good evidence whether this is happening in vaccinated humans (Doerfler, 2021). While we don’t whether the spike mRNA is inserted into our genomes, and, if so, whether that DNA would be expressed or suppressed, we do have evidence that spike proteins are expressed for at least two months following Covid-19 mRNA vaccination.As Danice Hertz, MD has written in a response to an article about Long Covid, “There are many thousands of people who have suffered a similar neurological syndrome as a result of receiving a Covid vaccine. I am one of those people and have severe neuropathic pain from head to toe as well as tinnitus, dizziness, imbalance, blurred vision, fatigue, headaches for 14 months now. Many of us have been diagnosed with small fiber neuropathy, dysautonomia and mast cell activation syndrome. It is time that these vaccine reactions be acknowledged, and that research be conducted to help understand the mechanism of injury so better treatments can be available to help those like me who have suffered terrible injury from the vaccines” (George, 2022). Recently, Gregory Poland, MD, director of the Mayo Clinic’s Vaccine Research Group in Rochester, Minnesota, reported his severe tinnitus after receiving the second dose of a mRNA covid-19 vaccine. ”It was like someone suddenly blew a dog whistle in my ear,” Poland told MedPage Today. ”It has been pretty much unrelenting.” Since then, Poland said he has been experiencing what he describes as life-altering tinnitus. Commenting on his symptoms, he ”can only begin to estimate the number of times I just want to scream because I can’t get rid of the noise or how many hours of sleep I’ve lost,” (Henderson, 2022).In this analysis and case study of vaccine induced autoimmune disease, I’ll first assume that the vaccine was manufactured correctly, and transported and stored appropriately so that the vaccine itself was normal. This, of course, is a big assumption given recent reports of manufacturing irregularities at the vaccine manufacturing facilities (Kansteiner, 2021). Because the VAERS vaccine adverse event reporting system in the US is voluntary, and few physicians or individuals who have been vaccinated report their injuries (Vaccines and The National Vaccine Injury Compensation Program, https://dash.harvard.edu/handle/1/9453695), the rate of vaccine induced injury is unknown. “The concern of some physicians about potential legal liability for an adverse event following vaccination was cited by some participants as a reason for underreporting in VAERS” (IOM, 1997). According to Ross et al (2010), “less than 0.3% of all adverse drug events and 1-13% of serious events are reported to the Food and Drug Administration (FDA). Likewise, fewer than 1% of vaccine adverse events are reported” (Ross et al, 2010). The underreporting of AEs occurs for many different vaccines that are routinely used (Cunningham, 2010). The problem of underreported AEs is significant (about 85%) for all drugs, not just vaccines (Hazell and Shakir, 2006).Some studies have attempted to capture the true rate, such as that for vaccine induced myocarditis (Barda et al, 2021), but these studies are rare and are usually poorly executed, if only because the data base from which the adverse events are taken is of poor quality. Here’s part of the problem too: if one has been injured by the vaccine, symptomatic for tinnitus, vertigo, and brain fog, there are not ostensible or clinically measurable manifestations of the disease. Not displaying something such as facial paralysis, often errantly called Bell’s Palsey by physicians (Scorza and Finisterer, 2021), leads the clinician to order blood tests and perhaps an nMRI scan. Nothing will be found when the physician orders these tests. Using standard clinical measures without a semi-shotgun approach to assaying the patients exoproteosome, in search of autoantibodies, the clinician will find no problems with their patients and tell the patient, “It’s all in your head” (Boodman, 2018). In terms of doing research on vaccine induced injuries, according to an article in Science, “I’ve talked to a lot of clinicians and researchers at various universities, and they don’t want to touch it” (Couzin-Frankel and Vogel, 2022).According to the CDC, among 71,491 U.S. adults who were hospitalized with COVID-19, 27.8 percent were overweight and 50.2 were obese (Kompaniyets et al, 2021). The analysis included 148,494 patients who received a COVID-19 diagnosis at emergency departments or inpatient visits between April 1 and Dec. 31 across 238 hospitals. Thus, 78% of the people sampled in this study who were hospitalized because of Covid-19, 78% were overweight or obese. Those who were overweight or obese were more likely to require invasive mechanical ventilation. Obesity was also linked to increased risk for hospitalization and death, especially among those under age 65. As BMI rose, so did the risk, the CDC found. Obesity is a major risk factor for autoimmune disease (Versini et al, 2014), and obese patients with Covid-19 produce a majority of SARS-CoV-2-specific antibodies that are autoimmune and not neutralizing (Frasca et al, 2021). Among other problems, autoantibodies can destroy neutrophils (Shastri and Logue, 1993) and leave the patient with a diminished innate immune response to the virus.