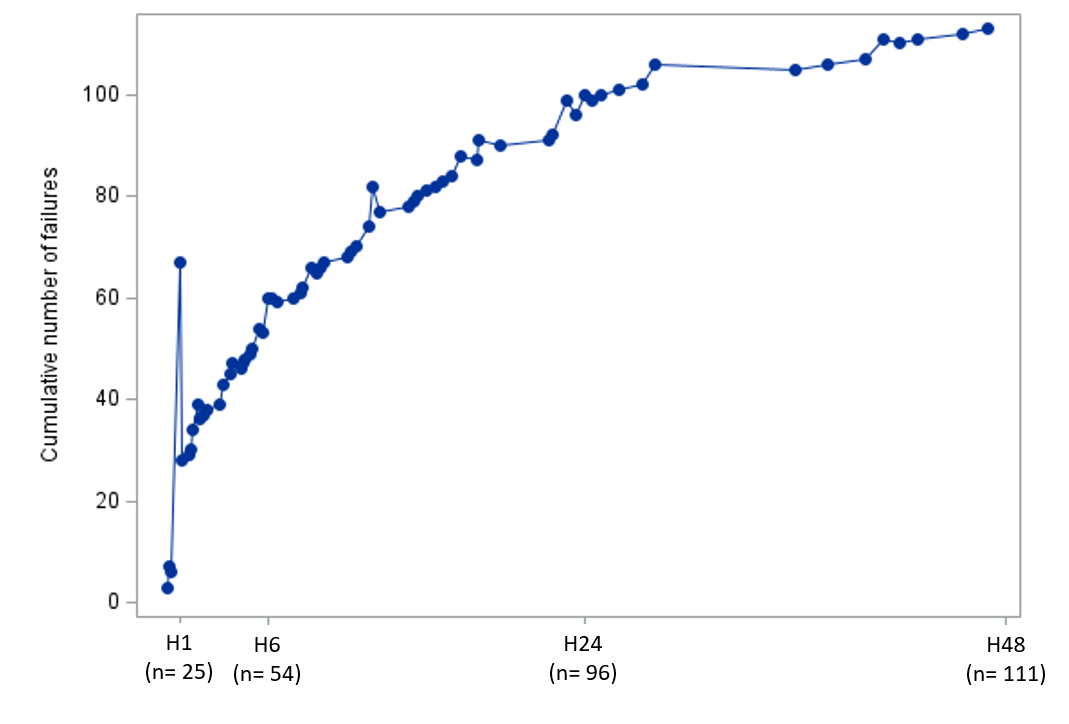
Introduction High flow nasal cannula (HFNC) is commonly used as first step respiratory support in infants with moderate-to-severe acute viral bronchiolitis (AVB). This device, however, fails to effectively manage respiratory distress in about a third of patients, and data are limited on determinants of patient response. The respiratory rate-oxygenation (ROX) index is a relevant tool to predict the risk for HFNC failure in adult patients with lower respiratory tract infections. The primary objective of this study was to assess the relationship between ROX indexes collected before and 1 hour after HFNC initiation, and HFNC failure occurring in the following 48 hours in infants with AVB. Method: This is an ancillary study to the multicenter randomized controlled trial TRAMONTANE 2, that included 286 infants of less than 6 months with moderate-to-severe AVB. Collection of physiological variables at baseline (H0), and 1 hour after HFNC (H1), included heart rate (HR), respiratory rate (RR), fraction of inspired oxygen (FiO 2), respiratory distress score (mWCAS), and pain and discomfort scale (EDIN). ROX was calculated as SpO 2/FiO 2 to RR. Predefined HFNC failure criteria included increase in respiratory distress score or respiratory rate, increase in discomfort, and severe apnea episodes. The accuracy of ROX index to predict HFNC failure was assessed using receiver operating curve analysis. Result: HFNC failure occurred in 111/286 (39%) infants, and for 56 (50% of the failure) of them within the first 6 hours. The area under the curve of ROX indexes at H0 and H1 were, respectively, 0.56 (95% CI 0.48-0.63, p =0.14), 0.56 (95% CI 0.49- 0.64, p =0.09). HFNC failure was associated with higher mWCAS score at H1 (p<0.01) and lower decrease in EDIN scale during the first hour of HFNC delivery (p = 0.02), but none of the physiological variables were predictive of HFNC failure. Conclusion: In this study, neither ROX index, nor physiological variables usually collected in infants with AVB had early discriminatory capacity to predict HFNC failure.